The Map of the Private Violence Virus
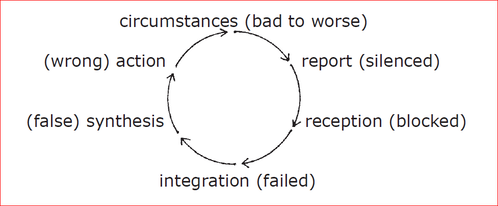
Violence synthesis and response patterns act like a family of infectious disorders, passed like a virus, usually parent to child but within many other relationships as well. The model shown is a map of the archetype viral pattern.
How the disease is transmitted:
The parent carries the virus contracted when he was a child. That the parent is affected become part of the circumstances of the child. The circumstances include private exposure to their parent, and the viral mandate (triggered by stress) causes the parent to present a painful episode to the child.
Next, the assailant tells the child not to tell. This component of the viral mandate attempts to silence the child’s report.
If the child’s capacity for report is stronger than the attempts to silence it, (if the child tells anyway) the assailant then turns to others who are in position to receive the child’s report, to try to persuade them to not believe the child. The viral behavior endeavors to block reception of report.
If reception is successfully blocked, the content of the child’s external report fails to be integrated by others, in that they disregard it . . . it is tossed into the conceptual garbage can.
Though the content of report has been rejected, the fact that is the event of the child’s external report is sorted (integrated) into the reality map (synthesis) of household members as bad behavior or even an assault against an innocent victim (the parent/assailant).
With synthesis distorted, the response by the family is to punish the child who made the report. The child may be separated from any who remain willing to receive the report. The child is prevented from making any change in circumstances to preclude avoidance of future painful episodes of this type.
All the instinctive and social behaviors designed to improve a situation and remedy pain are shown to actually make the situation worse. The concordant response within the child is to cease using those behaviors, relative to that type of event.
This programming goes deeper than that. The child’s brain is programmed to receive and integrate their own internal report in the same fashion as their external report was received and integrated by their providing family. The child’s awareness is trained to disregard the facts.
A pocket of unconsciousness has become established in the mind of the child, patterned after the unconsciousness in the family. Circumstances continue to be dangerous, perhaps more so now that “the coast is clear,” as it were, for all kinds of mayhem to occur.
The virus prompts the parent carrier to present a continuing series of destructive episodes, reinforcing the pattern of unconsciousness in the child. The child fails to make another report, both externally and internally.
The successful completion of this private violence disorder is a person who fails to gain safety in case of personal assault, and whose system of gaining safety generally is dismantled and not operating. Another name for this acquired unconsciousness is learned helplessness.
This acquired unconsciousness virus attacks safety in the same way that AIDS attacks health. Both Acquired Unconsciousness and Acquired Immune Deficiency Syndrome destroy the system by which a person achieves safety or health. AIDS creates cellular and systemic unconsciousness. Private violence creates unconsciousness in the child and the family.
The target area, type and intensity of the momentary pain presented in the destructive episode is a simple objective print (sometimes subject to multipliers) of the particular virus present in the carrier. The lasting damage done by the painful episode is a function of the success of the attacks on report, reception, integration, synthesis, and response options.
The episodes of assault on the Circle of Consciousness can be presented by persons other than the original source of the painful episode. Report silencing, reception blocking, faulty synthesis presentation, and the limiting of response opportunity can come from seemingly unrelated sources: co-offenders.
One Case History:
“A three year old boy reported injuries by his father. His grandmother received his report. Professional people investigated, asking questions all around. A psychiatrist issued a reception blocker, hired as legal document, stating that the boy was lying about the source of his injuries.
Social workers then failed to receive the boy’s report. The boy’s movement towards establishing safer circumstances with his grandmother was blocked and he was returned to private exposure to the father. The child soon died of abdominal injury. The child’s mother later stated she had heard the lethal assault, and that she witnessed the boy in acute physical distress for some hours before he died. She did not initiate medical attention.”
It is clear that the father did not act alone in causing the death of the boy. Many agents of the singular virus acted in concert to create the success of the disease.
The private violence infection is an intricate, coordinated, and multilateral attack upon personal and collective consciousness. In the unconscious space that is created in the human (the space wherein intelligence does no longer function), a viral print of the painful episode remains as a piece of subconscious programming, directing the human in future inhuman behavior.
When odds are too low that a particular body’s ability to build successful immunity before a disease has progressed to the point of serious damage or death, the human community of mind takes special note. Minds pool information, and consciousness acts to create improved immunity. Improved immunity, in this case, depends upon improved community.
How the disease is transmitted:
The parent carries the virus contracted when he was a child. That the parent is affected become part of the circumstances of the child. The circumstances include private exposure to their parent, and the viral mandate (triggered by stress) causes the parent to present a painful episode to the child.
Next, the assailant tells the child not to tell. This component of the viral mandate attempts to silence the child’s report.
If the child’s capacity for report is stronger than the attempts to silence it, (if the child tells anyway) the assailant then turns to others who are in position to receive the child’s report, to try to persuade them to not believe the child. The viral behavior endeavors to block reception of report.
If reception is successfully blocked, the content of the child’s external report fails to be integrated by others, in that they disregard it . . . it is tossed into the conceptual garbage can.
Though the content of report has been rejected, the fact that is the event of the child’s external report is sorted (integrated) into the reality map (synthesis) of household members as bad behavior or even an assault against an innocent victim (the parent/assailant).
With synthesis distorted, the response by the family is to punish the child who made the report. The child may be separated from any who remain willing to receive the report. The child is prevented from making any change in circumstances to preclude avoidance of future painful episodes of this type.
All the instinctive and social behaviors designed to improve a situation and remedy pain are shown to actually make the situation worse. The concordant response within the child is to cease using those behaviors, relative to that type of event.
This programming goes deeper than that. The child’s brain is programmed to receive and integrate their own internal report in the same fashion as their external report was received and integrated by their providing family. The child’s awareness is trained to disregard the facts.
A pocket of unconsciousness has become established in the mind of the child, patterned after the unconsciousness in the family. Circumstances continue to be dangerous, perhaps more so now that “the coast is clear,” as it were, for all kinds of mayhem to occur.
The virus prompts the parent carrier to present a continuing series of destructive episodes, reinforcing the pattern of unconsciousness in the child. The child fails to make another report, both externally and internally.
The successful completion of this private violence disorder is a person who fails to gain safety in case of personal assault, and whose system of gaining safety generally is dismantled and not operating. Another name for this acquired unconsciousness is learned helplessness.
This acquired unconsciousness virus attacks safety in the same way that AIDS attacks health. Both Acquired Unconsciousness and Acquired Immune Deficiency Syndrome destroy the system by which a person achieves safety or health. AIDS creates cellular and systemic unconsciousness. Private violence creates unconsciousness in the child and the family.
The target area, type and intensity of the momentary pain presented in the destructive episode is a simple objective print (sometimes subject to multipliers) of the particular virus present in the carrier. The lasting damage done by the painful episode is a function of the success of the attacks on report, reception, integration, synthesis, and response options.
The episodes of assault on the Circle of Consciousness can be presented by persons other than the original source of the painful episode. Report silencing, reception blocking, faulty synthesis presentation, and the limiting of response opportunity can come from seemingly unrelated sources: co-offenders.
One Case History:
“A three year old boy reported injuries by his father. His grandmother received his report. Professional people investigated, asking questions all around. A psychiatrist issued a reception blocker, hired as legal document, stating that the boy was lying about the source of his injuries.
Social workers then failed to receive the boy’s report. The boy’s movement towards establishing safer circumstances with his grandmother was blocked and he was returned to private exposure to the father. The child soon died of abdominal injury. The child’s mother later stated she had heard the lethal assault, and that she witnessed the boy in acute physical distress for some hours before he died. She did not initiate medical attention.”
It is clear that the father did not act alone in causing the death of the boy. Many agents of the singular virus acted in concert to create the success of the disease.
The private violence infection is an intricate, coordinated, and multilateral attack upon personal and collective consciousness. In the unconscious space that is created in the human (the space wherein intelligence does no longer function), a viral print of the painful episode remains as a piece of subconscious programming, directing the human in future inhuman behavior.
When odds are too low that a particular body’s ability to build successful immunity before a disease has progressed to the point of serious damage or death, the human community of mind takes special note. Minds pool information, and consciousness acts to create improved immunity. Improved immunity, in this case, depends upon improved community.
